A hysterosalpingogram (HSG) is a common diagnostic test used to evaluate the uterus and fallopian tubes. During an HSG test, an iodine-based dye is introduced through the cervix, and into the uterine cavity and fallopian tubes. A special type of x-ray is used to track the movement of the dye. By viewing the flow of the dye through the woman’s reproductive structures, practitioners can view the size, shape, and position of the uterus. They can also visualize any blockages in the fallopian tubes.
Why Is the HSG Test Necessary?
During ovulation, a mature egg is released from the ovary. It is then swept into one of the fallopian tubes where it will be available to meet sperm. If the egg is fertilized by sperm, the early embryo will then travel down the fallopian tube to the uterus. There, it may implant and result in a pregnancy. If one or both fallopian tubes are blocked, the sperm cannot access the egg. During an HSG test, dye that does not flow all the way through the fallopian tubes and spill into the abdominal cavity, indicates a blockage.
A hydrosalpinx can also be diagnosed with an HSG test. A hydrosalpinx is a collection of fluid in one or both fallopian tubes. The fluid collects because there is damage to the end of the fallopian tube. A previous pelvic infection, surgery or endometriosis can cause inflammation and scarring. A hydrosalpinx may need to be surgically removed prior to pregnancy.
An HSG test can also help diagnose other uterine issues that may have occurred before birth. Before a female child is born, the uterus begins developing from two separate structures, two uteruses and two cervixes that fuse together as the female fetus grows. Occasionally the two separate structures fail to fuse completely and will result in a uterine anomaly. As the uterus fills with dye during the HSG test, practitioners can very clearly see the size, shape and whether there are any anomalies. There are multiple variations of uterine anomalies that can be diagnosed with an HSG test. A septate, bicornuate and didelphic uterus are all examples of uterine anomalies that can be discovered with an HSG test.
What Is the Procedure Like?
The HSG procedure is usually a short, five-to-ten-minute examination performed either in a procedure room or imaging center. The patient will be instructed to lay down on a table with their feet placed in stirrups.
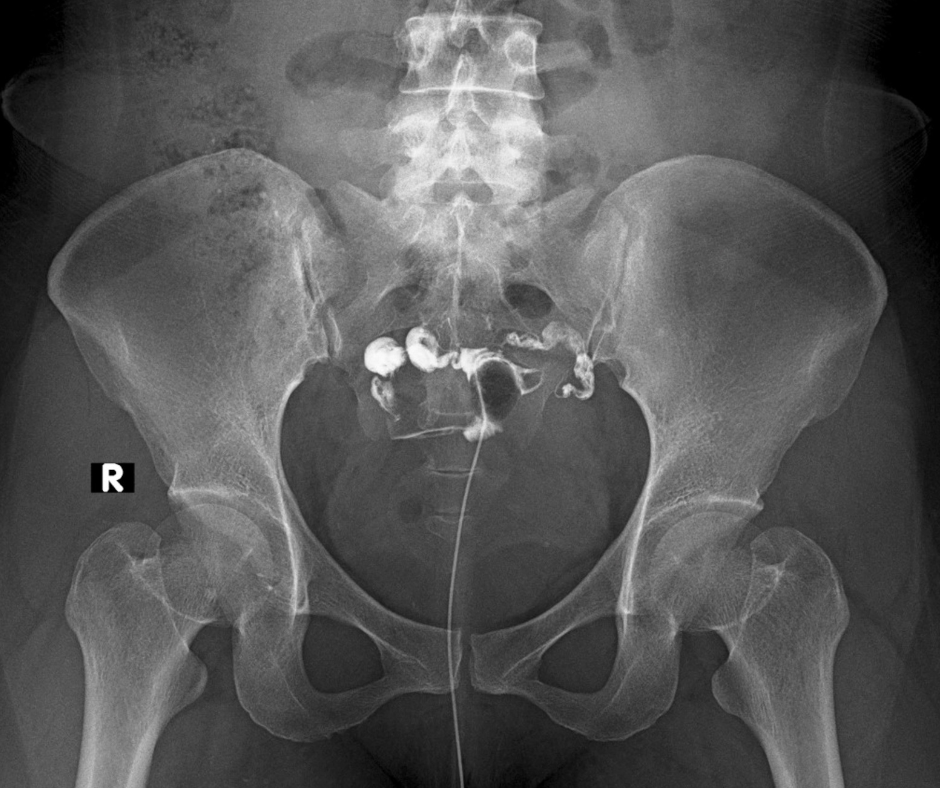
Once in the correct position, an x-ray technician will bring over a large machine called a fluoroscope and take an image of the pelvis. Once the machine has been placed in the correct position, a practitioner will place a speculum in the vagina to visualize the cervix, the bottom part of the uterus. A thin plastic tube called a catheter is placed inside the cervix. Once the catheter is in position, the practitioner will begin to administer the dye through the catheter. The dye will then flow into the uterus and fallopian tubes.
Meanwhile, the fluoroscope will be taking images while the dye is moving. If the fallopian tubes are both open, the dye will move through the tubes and spill into the abdominal cavity on both the right and left sides. If one of the tubes is blocked or surgically removed, the dye will not spill from the end of the fallopian tube.
Once the uterine cavity is visualized and the status of both tubes is observed, the exam will conclude. The speculum will be removed, and the patient may feel some watery discharge as they sit up. The procedure may cause some cramping and pressure, but the cramping usually subsides shortly after the exam. You can usually go back to work or school right after the procedure.
Can HSG Be Used to Treat Infertility?
While HSG is primarily a diagnostic tool, some evidence has surfaced suggesting it might also work as a form of treatment. It seems that women who have had “tubal flushing” (HSG contrast dye pushed through the fallopian tubes) conceive more often than those who do not. Thirteen randomized controlled trials involving 2,494 women were brought together by Cochrane review authors. They looked at pregnancy rates for women who had not been able to get pregnant. These women had experienced six months of unprotected intercourse. These women received HSG with oil- or water-soluble dye or had no intervention at all.
The evidence suggested that women who had HSG with an oil-soluble medium had increased rates of pregnancy. In fact, the chance of pregnancy increased from 17% to between 29% and 55% after HSG with oil-based dye. HSG using water-soluble dye did not have the same effect. The researchers described the quality of the data as “low” or “very low,” meaning the study is far from conclusive.
However, another study conducted in the Netherlands in 2017 and published in the New England Journal of Medicine found a statistically significant difference in pregnancy rates. This difference was observed for women who had HSG with oil-soluble or water-soluble dye.
This study, dubbed the H2Oil study, looked at 1,119 women under 38 years of age who had been trying to conceive unsuccessfully for an average of 18 months. Of those who received the oil-based dye, 40% achieved successful pregnancies within six months compared with 29% who received the water-based dye.
Why Does the HSG Test Work?
Scientists still cannot answer exactly why having HSG with an oil-based dye appears to improve fertility. One idea would be that the “tubal flushing” helps to clear debris and mucus buildup in fallopian tubes. Another thought is that the oil-based dye improves endometrial receptivity. Regardless of the reason, the HSG test is significantly less expensive and less invasive than IVF with a very low risk of complication. Additionally, it can improve clinical pregnancy rates. While the evidence isn’t bulletproof now, perhaps additional research can shed more light on these exciting findings.

